Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Jesus Vicente de Julián-Ortiz | -- | 1514 | 2023-05-19 21:53:17 | | | |
| 2 | Conner Chen | Meta information modification | 1514 | 2023-05-22 04:44:54 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Taléns-Visconti, R.; De Julián-Ortiz, J.V.; Vila-Busó, O.; Diez-Sales, O.; Nácher, A. Intranasal Drug Administration in Alzheimer-Type Dementia. Encyclopedia. Available online: https://encyclopedia.pub/entry/44584 (accessed on 24 July 2026).
Taléns-Visconti R, De Julián-Ortiz JV, Vila-Busó O, Diez-Sales O, Nácher A. Intranasal Drug Administration in Alzheimer-Type Dementia. Encyclopedia. Available at: https://encyclopedia.pub/entry/44584. Accessed July 24, 2026.
Taléns-Visconti, Raquel, Jesus Vicente De Julián-Ortiz, Ofelia Vila-Busó, Octavio Diez-Sales, Amparo Nácher. "Intranasal Drug Administration in Alzheimer-Type Dementia" Encyclopedia, https://encyclopedia.pub/entry/44584 (accessed July 24, 2026).
Taléns-Visconti, R., De Julián-Ortiz, J.V., Vila-Busó, O., Diez-Sales, O., & Nácher, A. (2023, May 19). Intranasal Drug Administration in Alzheimer-Type Dementia. In Encyclopedia. https://encyclopedia.pub/entry/44584
Taléns-Visconti, Raquel, et al. "Intranasal Drug Administration in Alzheimer-Type Dementia." Encyclopedia. Web. 19 May, 2023.
Copy Citation
Alzheimer-type dementia (ATD) treatments face limitations in crossing the blood–brain barrier and systemic adverse effects. Intranasal administration offers a direct route to the brain via the nasal cavity’s olfactory and trigeminal pathways.
intranasal delivery
Alzheimer
blood–brain barrier
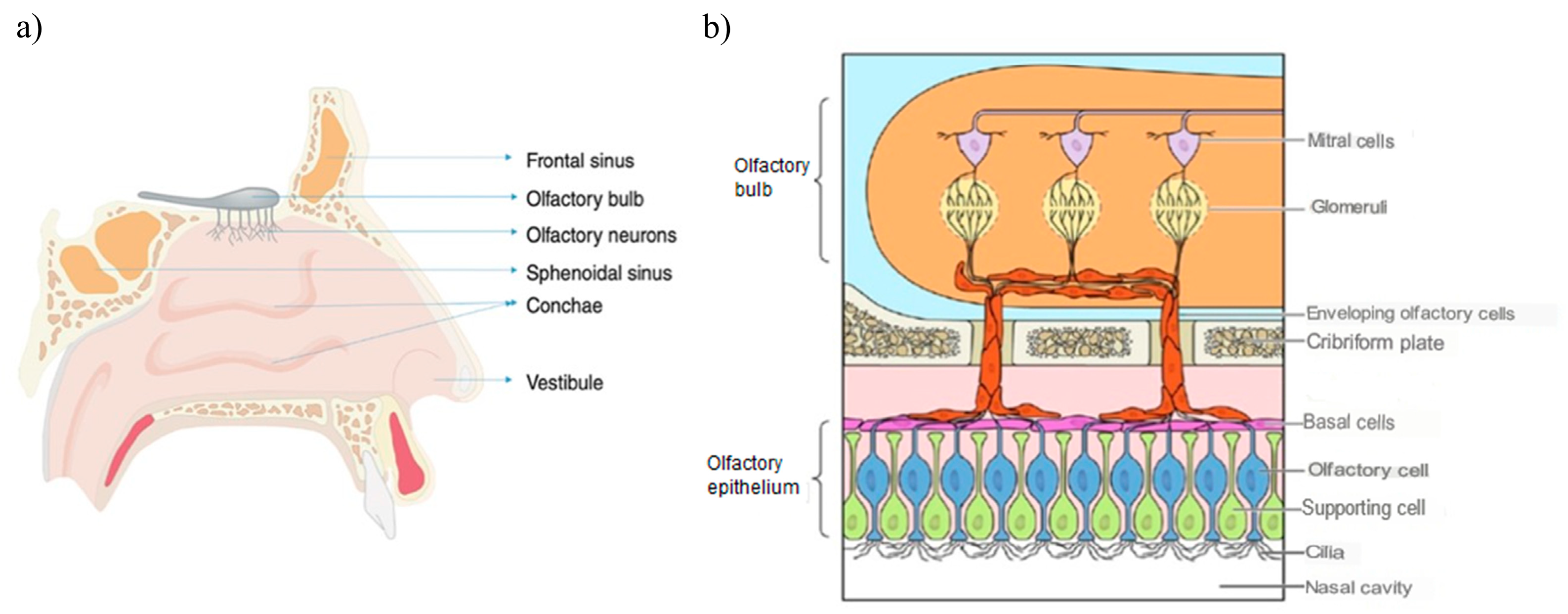
1. Nasal Cavity Anatomy
The main functions of the nasal cavity are breathing and smell, and, in addition, it exerts a protective action of filtering, warming and humidifying the inhaled air before it reaches the lower respiratory tract [1]. Likewise, it is composed of two symmetrical cavities that are divided by the nasal septum and lined with a layer of mucosa. These cavities in turn are divided into three regions:
- Vestibular region: This is the most anterior area, and contains nasal hairs to filter inhaled particles and the main cell type is squamous epithelial cells. In this region, drug absorption is very limited [2].
- Respiratory region: This is the area with the largest surface (about 130 cm2) and the most vascularity, which makes it an ideal place for the systemic absorption of drugs. It encompasses the lateral walls of the nostrils, including the protruding nasal turbinates. There are four main cell types: goblet, ciliated, non-ciliated columnar and basal. In addition, the respiratory region is innervated by the maxillary and ophthalmic branches of the trigeminal nerve (V1, V2) [3].
- Olfactory region: This is located on the roof of the nasal cavity and covers only 10% of the total nasal area. There are different types of cells: basal cells, olfactory nerve cells, support cells, cilia and trigeminal neurons. In addition, the olfactory region facilitates the transport of drugs to the brain having a direct connection with the brain through the olfactory and trigeminal neurons [4].
Figure 1 illustrates the anatomy of the nasal cavity and provides a schematic representation of the olfactory region.
2. Intranasal Absorption
The first step in drug absorption from the nasal cavity is to cross the mucus layer. Mucin, which is the major mucus protein capable of binding solutes, hinders drug diffusion. Non-ionized, lipophilic and small particles easily pass through this layer of mucus. Thus, the molecular weight and lipophilicity of drugs can have a large impact on the rate and degree of nasal absorption of drugs. However, other physicochemical properties of the drug and the formulation must also be considered, as well as some physiological factors of the nose, which may also influence the bioavailability and transport of the drug from the nose to the brain [7].
Figure 2 summarizes the main factors that influence the nasal absorption of drugs administered by this route.
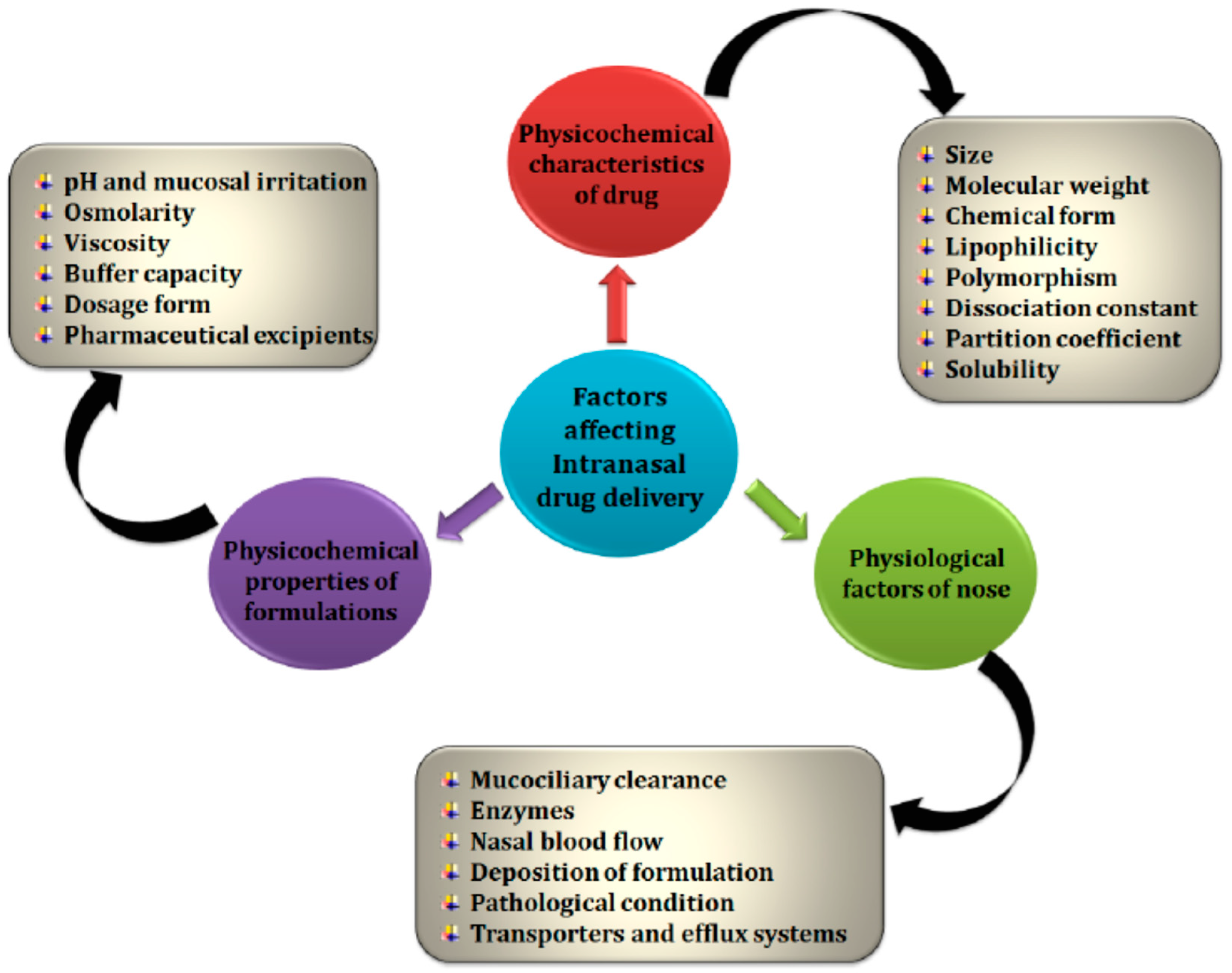
Figure 2. Factors affecting absorption through the nasal route [7].
Once through the mucus, different mechanisms of absorption can be followed through the nasal mucosa: transcellular diffusion, paracellular transport, endocytic vesicle-mediated transport and carrier-mediated transport. Transcellular diffusion is the main mechanism of absorption and is the most suitable for lipophilic and low molecular weight molecules [8][9]. Figure 3 schematically represents the different mechanisms of absorption through the nasal mucosa.
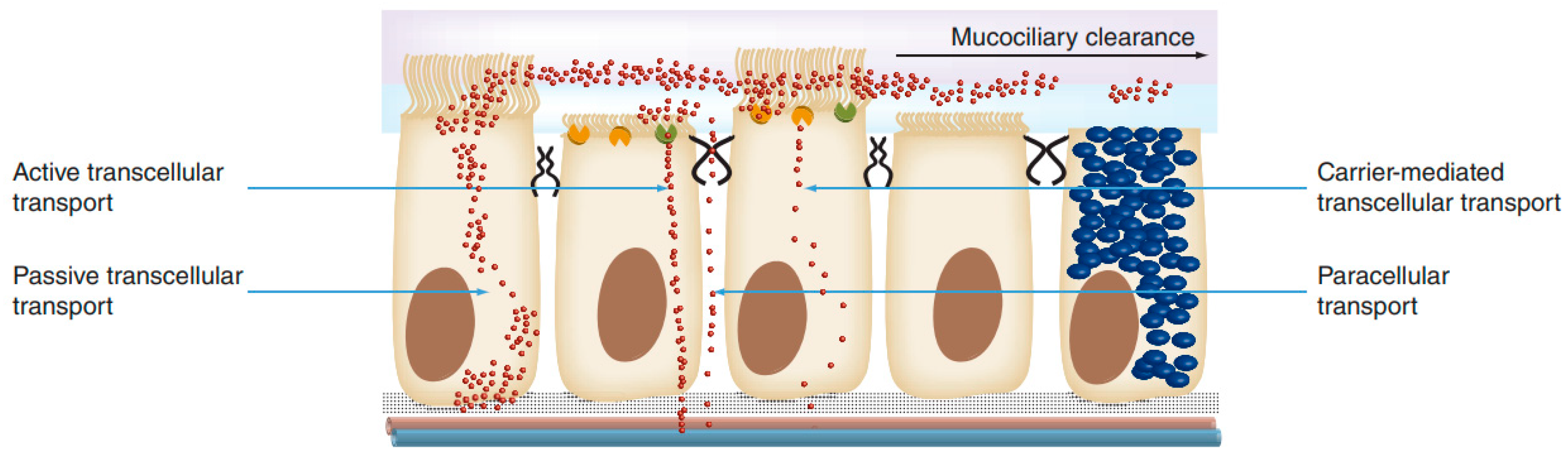
Figure 3. Mechanisms of drug absorption across the nasal epithelium [5].
3. Nose–Brain Absorption Pathways
- (a)
-
Direct Absorption Mechanism
-
Olfactory Sensory Neurons
The olfactory nerve pathway is a direct and primary route of drug transport from the nasal cavity to the brain, preventing its passage through the BBB. When the drug reaches the olfactory receptors after passing through the nasal mucosa, there are two transport mechanisms to the brain: the intracellular route, in which the drug is taken up by the olfactory neurons through a process of endocytosis, and the extracellular route, in which the drug crosses the nasal epithelium through the tight junctions between the olfactory nerves and the supporting cells [10].
In both cases, the molecules travel through the cribriform plate, which separates the brain from the nasal cavity, to enter the olfactory bulb and the CSF. Subsequently, the drug can be distributed from the CSF to the brain by mixing with the interstitial fluid of the brain. The intracellular route requires from hours to days for the active fraction to reach the different regions of the brain and is adequate for the passage of lipophilic molecules, while the extracellular route only requires a few minutes for the active fraction to reach the brain and is suitable for the passage of hydrophilic molecules [11]. Figure 4 schematically represents the intranasal transport of drugs through the olfactory route to the CNS by the intracellular and extracellular route.
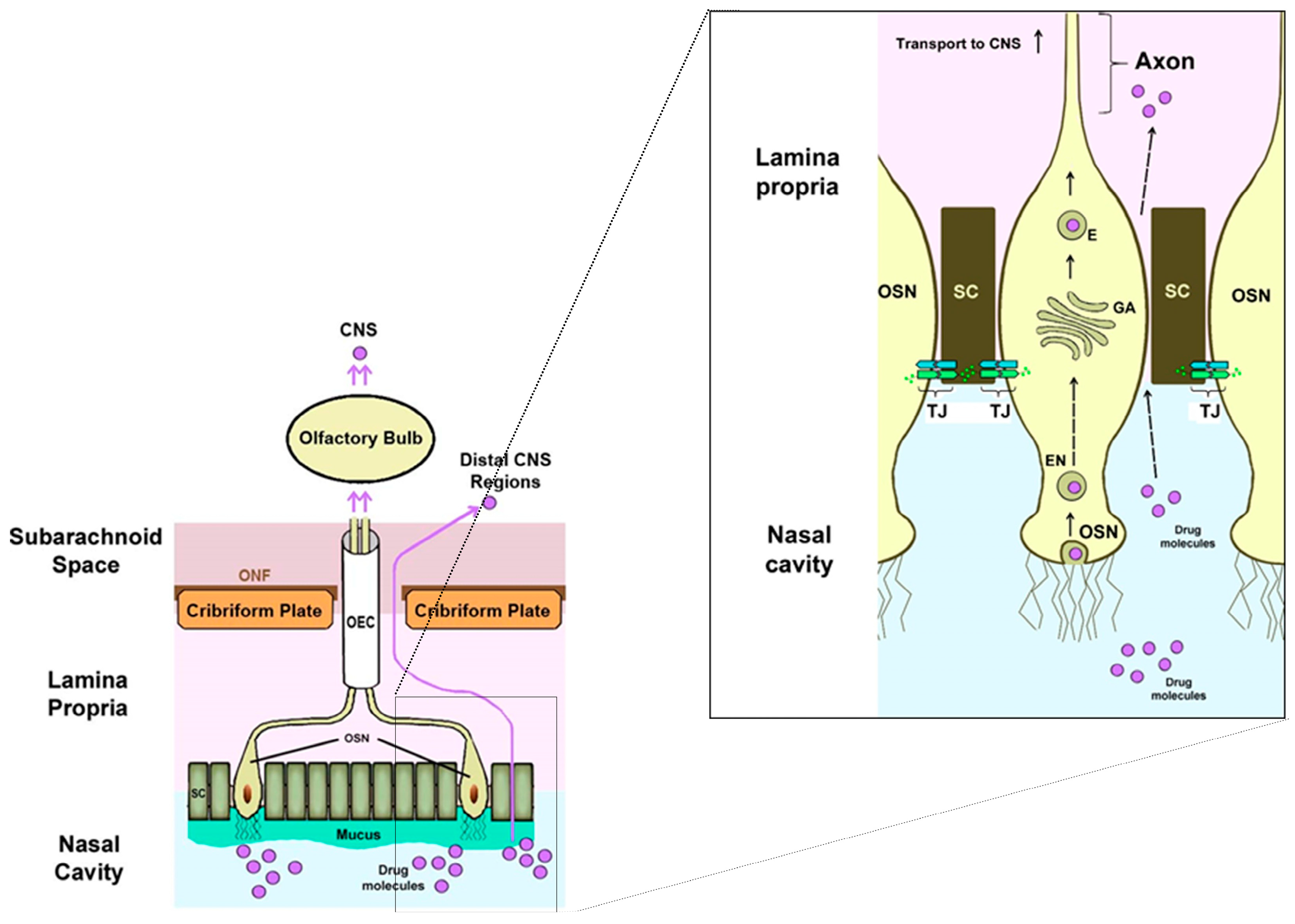
Figure 4. Intranasal transport of drugs through the olfactory route to the CNS by intracellular and extracellular routes [10].
-
Trigeminal Neurons
Both the respiratory and olfactory epithelium are supplied with trigeminal nerves (Figure 5). Branches from the ophthalmic division (V1) of the trigeminal nerve innervate the dorsal and anterior part of the nasal mucosa, and those from the maxillary division (V2) innervate the turbinates.
Once the drug has diffused through the mucosa, it allows its transport directly to the brainstem at the level of the pons, avoiding its passage through the BBB. Transport through the trigeminal route can also occur intracellularly or extracellularly, as occurs with olfactory neurons [12].
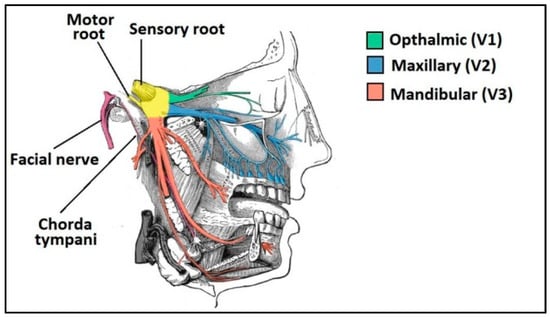
Figure 5. Innervation of the trigeminal nerve in the nasal cavity [13].
- (b)
-
Indirect Absorption Mechanism: The Systemic Route
When a drug is deposited in the nasal cavity and depending on its residence time, a part of it can be absorbed and enter the systemic circulation due to the rich vasculature of the respiratory epithelium and reach the brain through the BBB. This is a secondary route of drug transport to the brain after nasal administration [14].
Small lipophilic molecules gain access to the bloodstream and penetrate the BBB much more easily than high molecular weight and hydrophilic molecules. In addition, the active substances that use this route undergo renal and hepatic metabolism, so that the amount of drug that finally reaches the brain is very low and depends on the partition coefficient (0.5–6.0) and the molecular weight of the drug (<500 Da). It also leads to a higher incidence of unwanted side effects in other peripheral organs [15].
Figure 6 schematically represents the structure of the nasal cavity and the different mechanisms of drug transport through the nasal mucosa to the brain.
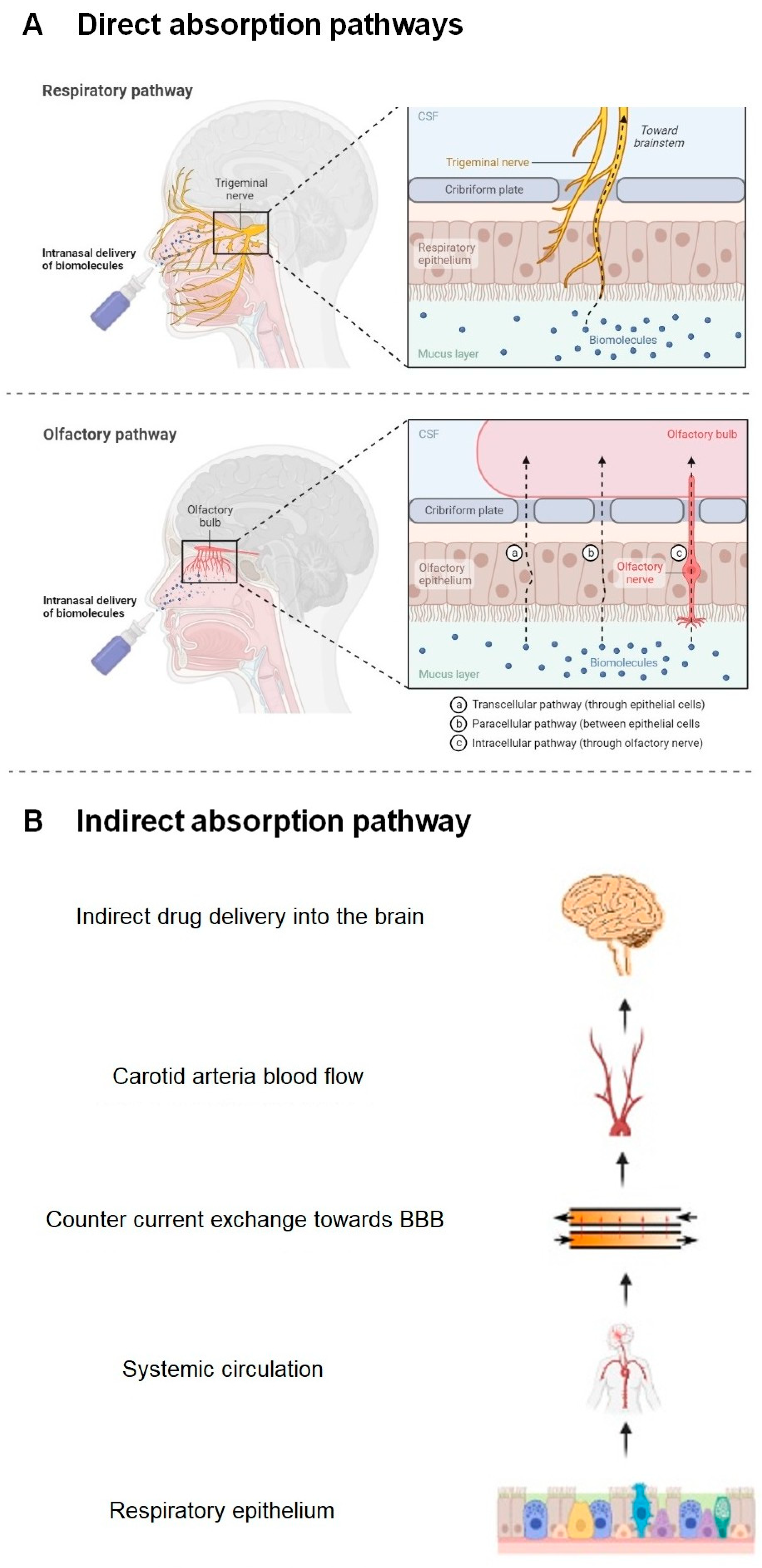
Figure 6. Schematic representation of the structure of the nasal cavity and the mechanisms of drug absorption through the nasal mucosa to the brain. (A) Direct absorption mechanism through olfactory nerve and trigeminal route. (B) Indirect absorption mechanism by systemic route [16].
4. Advantages and Disadvantages of the Nasal Route
To date, numerous techniques have been developed to circumvent the BBB and improve drug delivery to the brain, including invasive techniques, such as surgical exposure or intrathecal and intraventricular routes of administration.
The intranasal route offers a non-invasive strategy to bypass the BBB and provide direct drug access to the brain in a short period of time, as it has a direct connection to the brain through neural channels. In addition, the nasal cavity has a large number of blood vessels with rapid blood flow and has a large available surface area for absorption. For this reason, it offers other advantages such as rapid drug absorption, avoidance of hepatic metabolism and easy administration, which increases patient compliance [17].
However, there are several obstacles that can limit absorption of drug through this pathway, such as poor drug permeability from the nasal mucosa, mucociliary clearance, enzymatic degradation of the drug, low drug residence time and possible toxicity that the formulation or drug can produce on the nasal mucosa. In addition, due to the limited volume of application through this route, the dose of the drug may be limited depending on its solubility in the vehicle, so it will only be applicable to potent drugs that allow obtaining sufficient pharmacological effect at low doses or by using dry powders. Likewise, it would be convenient to reserve this route for those active principles with a wide therapeutic margin due to the possible inaccuracy of the dosage after administration. All these characteristics make it difficult to obtain bioavailability into the brain via the intranasal route [2]. For this reason, numerous technological strategies have been investigated to overcome these drawbacks and improve the bioavailability of drugs administered intranasally, which will be detailed later.
Table 1 indicates the main advantages and disadvantages associated with the administration of drugs through the nose.
Table 1. Advantages and drawbacks of nasal drug administration.
| Advantages | Disadvantages |
|---|---|
|
|
References
- Sobiesk, J.L.; Munakomi, S. Anatomy, Head and Neck, Nasal Cavity; StatPearls Publishing: Treasure Island, FL, USA, 2022.
- Akel, H.; Ismail, R.; Csóka, I. Progress and perspectives of brain-targeting lipid-based nanosystems via the nasal route in Alzheimer’s disease. Eur. J. Pharm. Biopharm. 2020, 148, 38–53.
- Lobaina Mato, Y. Nasal route for vaccine and drug delivery: Features and current opportunities. Int. J. Pharm. 2019, 572, 118813.
- Lee, D.; Minko, T. Nanotherapeutics for Nose-to-Brain Drug Delivery: An Approach to Bypass the Blood Brain Barrier. Pharmaceutics 2021, 13, 2049.
- Agu, R.U. Challenges in nasal drug absorption: How far have we come? Ther. Deliv. 2016, 7, 495–510.
- Dando, S.J.; Mackay-Sim, A.; Norton, R.; Currie, B.J.; St John, J.A.; Ekberg, J.A.; Batzloff, M.; Ulett, G.C.; Beacham, I.R. Pathogens penetrating the central nervous system: Infection pathways and the cellular and molecular mechanisms of invasion. Clin. Microbiol. Rev. 2014, 27, 691–726.
- Dhas, N.L.; Kudarha, R.R.; Mehta, T.A. Intranasal Delivery of Nanotherapeutics/Nanobiotherapeutics for the Treatment of Alzheimer’s Disease: A Proficient Approach. Crit. Rev. Ther. Drug Carrier Syst. 2019, 36, 373–447.
- Riccardi, C.; Napolitano, F.; Montesarchio, D.; Sampaolo, S.; Melone, M.A.B. Nanoparticle-Guided Brain Drug Delivery: Expanding the Therapeutic Approach to Neurodegenerative Diseases. Pharmaceutics 2021, 13, 1897.
- Poovaiah, N.; Davoudi, Z.; Peng, H.; Schlichtmann, B.; Mallapragada, S.; Narasimhan, B.; Wang, Q. Treatment of neurodegenerative disorders through the blood-brain barrier using nanocarriers. Nanoscale 2018, 10, 16962–16983.
- Erdő, F.; Bors, L.A.; Farkas, D.; Bajza, Á.; Gizurarson, S. Evaluation of intranasal delivery route of drug administration for brain targeting. Brain Res. Bull. 2018, 143, 155–170.
- Selvaraj, K.; Gowthamarajan, K.; Reddy-Karri, V.V.S. Nose to brain transport pathways an overview: Potential of nanostructured lipid carriers in nose to brain targeting. Artif. CellsNanomed. Biotechnol. 2018, 46, 2088–2095.
- Bahadur, S.; Pardhi, D.M.; Rautio, J.; Rosenholm, J.M.; Pathak, K. Intranasal Nanoemulsions for Direct Nose-to-Brain Delivery of Actives for CNS Disorders. Pharmaceutics 2020, 12, 1230.
- The Mandibular Division of the Trigeminal Nerve (CNV3)—TeachMeAnatomy. Available online: https://teachmeanatomy.info/head/nerves/mandibular-nerve/ (accessed on 28 March 2023).
- Bourganis, V.; Kammona, O.; Alexopoulos, A.; Kiparissides, C. Recent advances in carrier mediated nose-to-brain delivery of pharmaceuticals. Eur. J. Pharm. Biopharm. 2018, 128, 337–362.
- Bicker, J.; Fortuna, A.; Alves, G.; Falcão, A. Nose-to-brain Delivery of Natural Compounds for the Treatment of Central Nervous System Disorders. Curr. Pharm. Des. 2020, 26, 594–619.
- Cunha, S.; Forbes, B.; Sousa Lobo, J.M.; Silva, A.C. Improving Drug Delivery for Alzheimer’s Disease Through Nose-to-Brain Delivery Using Nanoemulsions, Nanostructured Lipid Carriers (NLC) and in situ Hydrogels. Int. J. Nanomed. 2021, 16, 4373–4390.
- Fonseca, L.C.; Lopes, J.A.; Vieira, J.; Viegas, C.; Oliveira, C.S.; Hartmann, R.P.; Fonte, P. Intranasal drug delivery for treatment of Alzheimer’s disease. Drug Deliv. Transl. Res. 2021, 11, 411–425.
More
Information
Subjects:
Neurosciences
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
1.2K
Revisions:
2 times
(View History)
Update Date:
22 May 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No